Food-Based Dietary Guidelines around the World: Eastern Mediterranean and Middle Eastern Countries


Abstract
:1. Introduction
2. Materials and Methods
3. Results
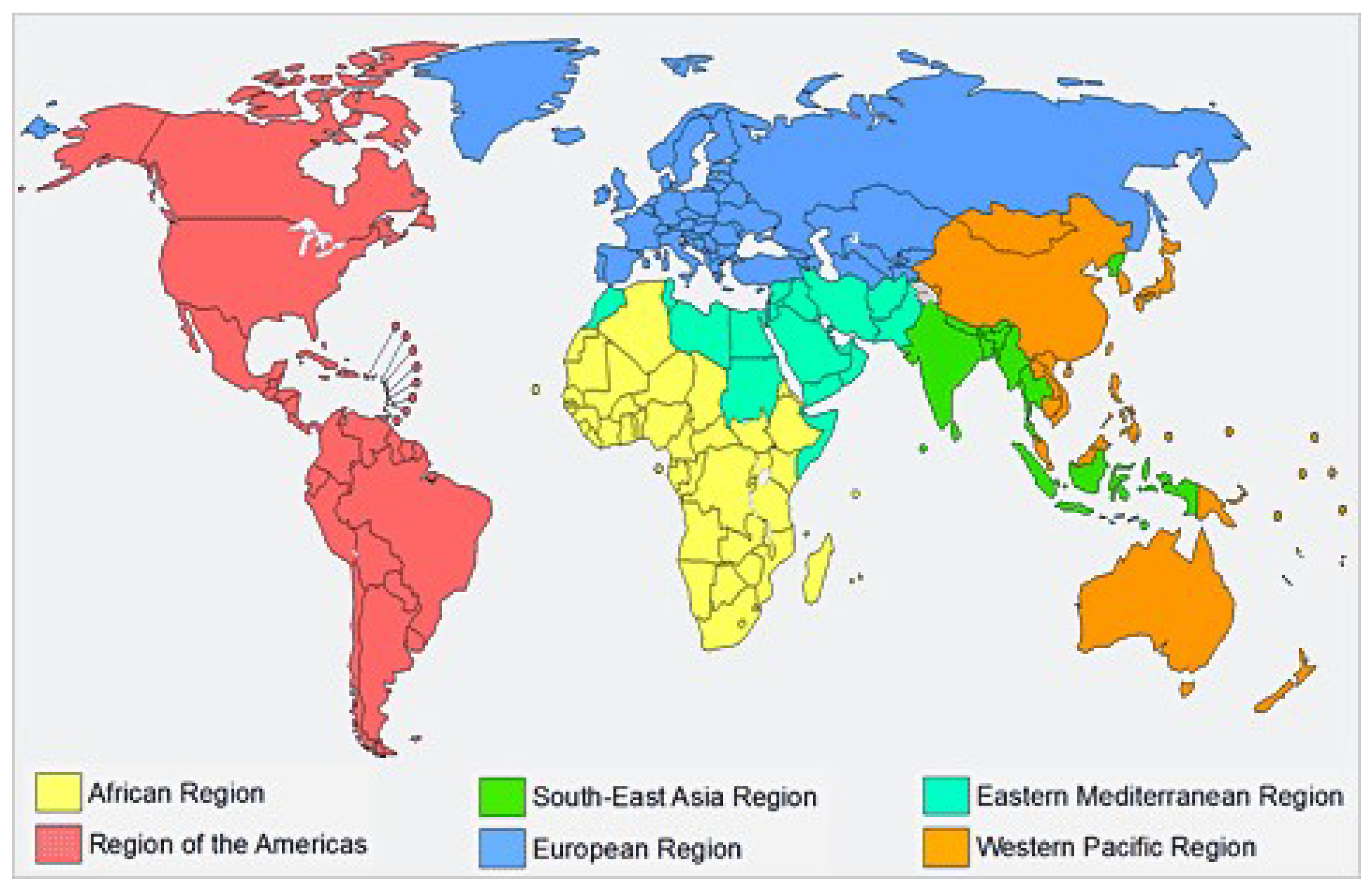
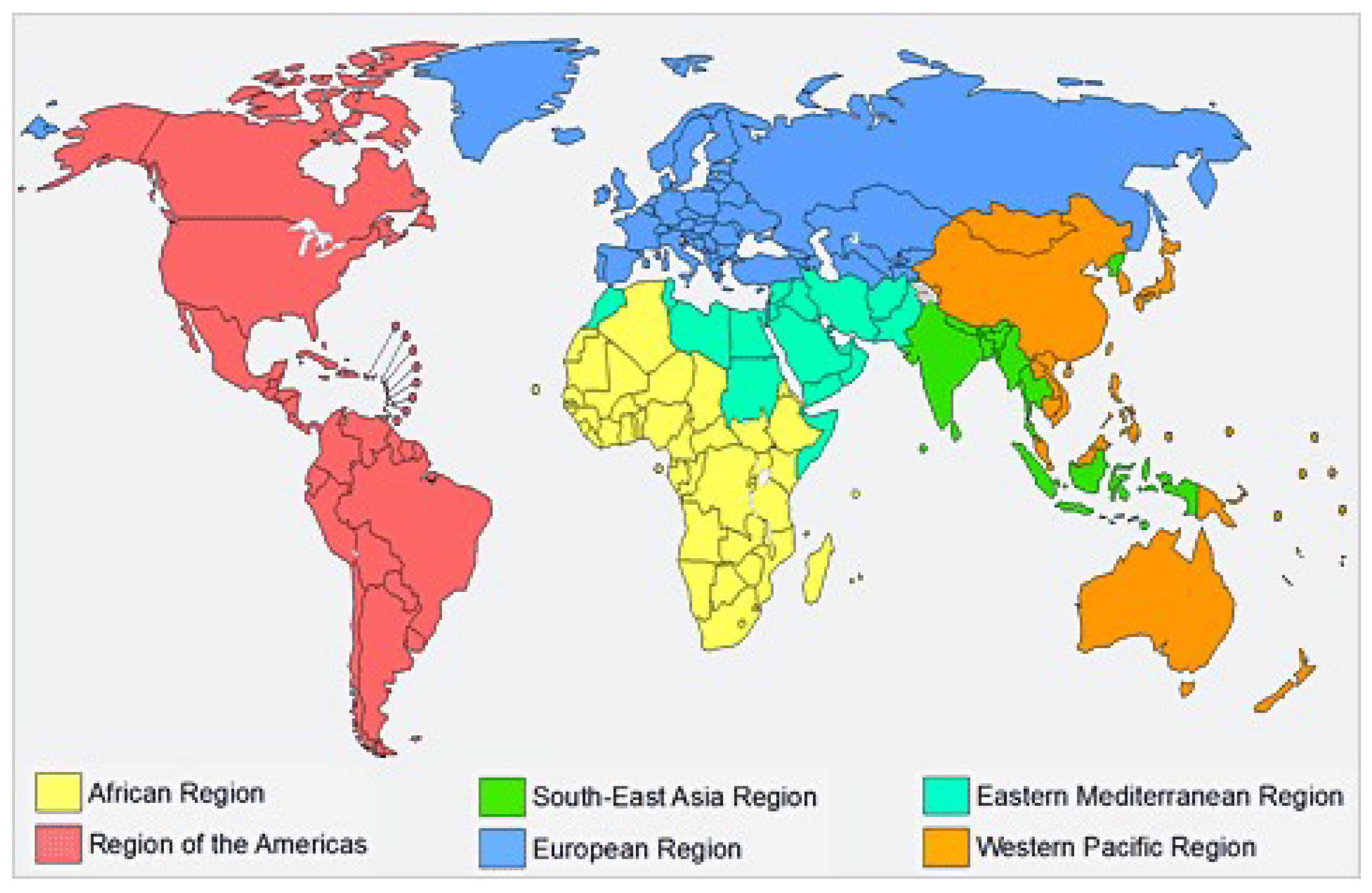
3.1. Geographic Distribution of the Studied Countries
3.2. Promoting a Healthy Diet for the WHO EMRO: User-Friendly Guide
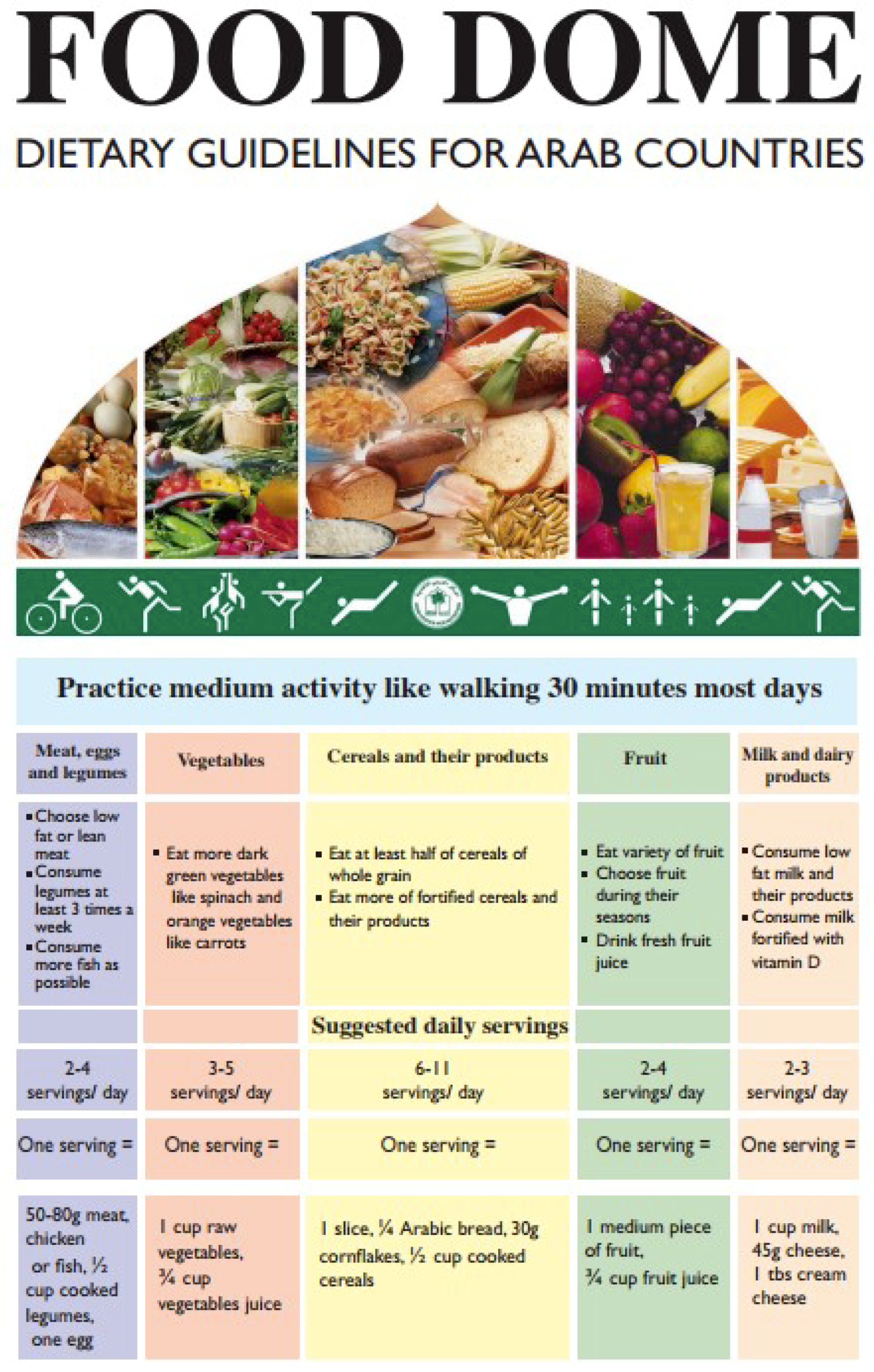
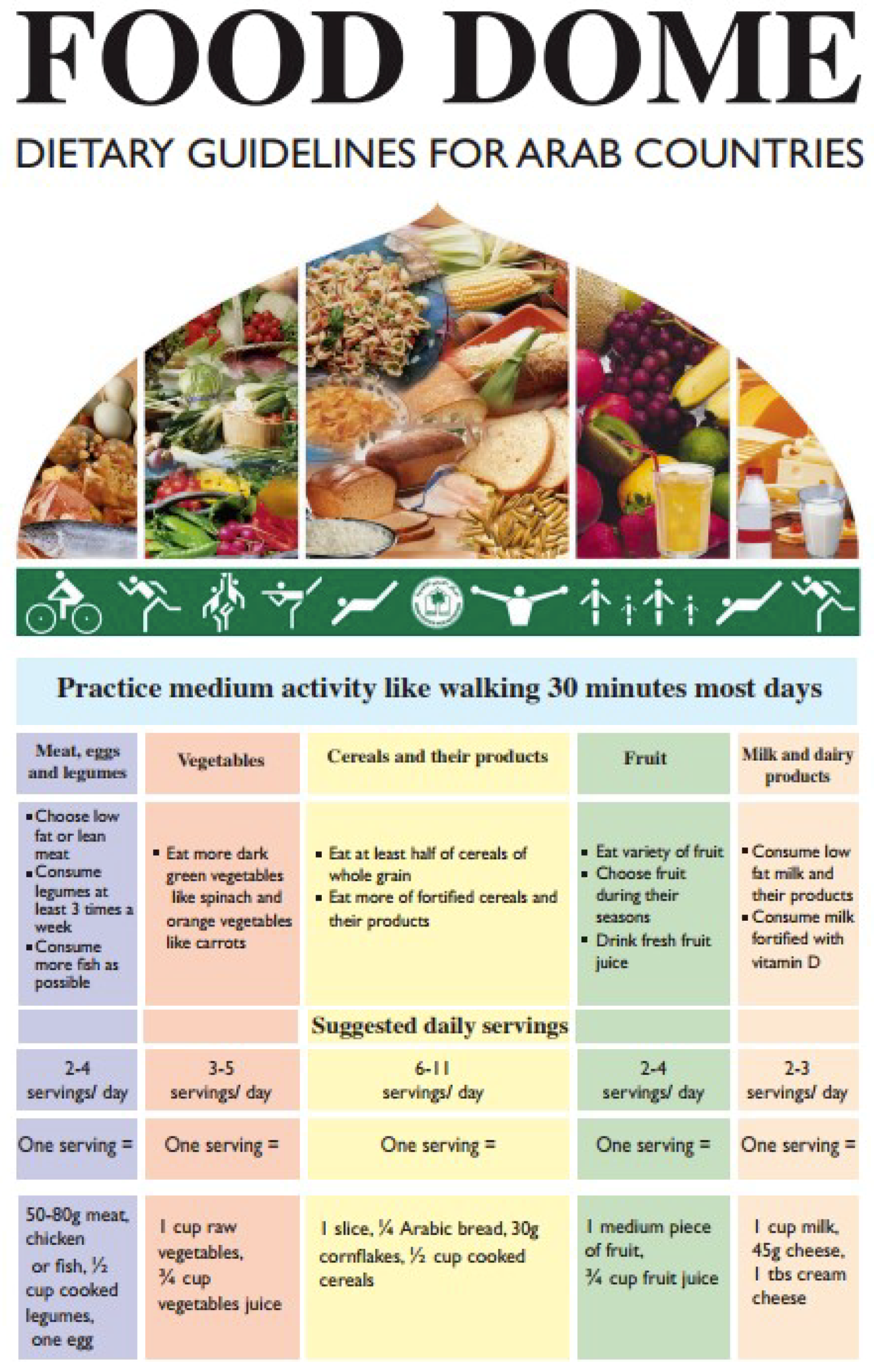
3.3. Food Dome Dietary Guidelines for Arab Countries
3.4. Food-Based Dietary Guidelines for Arab Gulf Countries
3.5. Food Guide Illustration Shapes
3.6. Language Used
3.7. Additional Information
3.8. Foods Pictured in the Graphics
3.9. Food Grouping
3.10. Salt Intake
3.11. Lifestyle, Physical Activity and other Healthy Behaviours
3.12. Specific Population Subgroups
4. Discussion
4.1. Specific Nutritional Characteristics of EMRO FBDGs
4.2. Special Recommendations Addressed to Local Environmental and Hygiene Peculiarities
4.3. EMRO FBDGs Pictures and Food Grouping
4.4. Messages on Healthy Lifestyles
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Smitasiri, S.; Uauy, R. Beyond recommendations: Implementing food-based dietary guidelines for healthier populations. Food Nutr. Bull. 2007, 28, S141–S151. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization; Food and Agriculture Organization (WHO/FAO). Expert Report: Diet, Nutrition and Prevention of Chronic Diseases; Report of A Joint WHO/FAO Expert Consultation; WHO Technical Report Series 916; WHO/FAO: Geneva, Switzerland, 2003. [Google Scholar]
- Musaiger, A.O.; Hassan, A.S. The paradox of nutrition-related diseases in the Arab countries: The need for action. Int. J. Environ. Res. Public Health 2011, 8, 3637–3671. [Google Scholar] [CrossRef] [PubMed]
- Musaiger, A.O. Food Consumption Patterns in the Eastern Mediterranean Countries; Arab Center for Nutrition: Manama, Bahrain, 2011. [Google Scholar]
- World Health Organization, Regional Office for the Eastern Mediterranean. Noncommunicable Diseases in the Eastern Mediterranean Region. Available online: https://apps.who.int/iris/handle/10665/250371WorldHealthOrganization/Eastern (accessed on 26 April 2019).
- Galal, O. The nutrition transition in Egypt: Obesity, undernutrition and the food consumption context. Public Health Nutr. 2002, 5, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Madanat, H.N.; Troutman, K.P. The nutrition transition in Jordan: The political, economic and food consumption context. Promot. Educ. 2008, 15, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.W.; Zaghlool, S. The prevalence and trends of overweight, obesity and nutrition-related non-communicable disease in the Arab Gulf states. Obes. Rev. 2011, 12, 1–13. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Framework for Health Information Systems and Core Indicators for Monitoring Health Situation and Health System Performance 2018. Available online: http://applications.emro.who.int/docs/EMROPUB_2018_EN_20620.pdf?ua=1 (accessed on 26 April 2019).
- Frost, A.; Wilkinson, M. An assessment of the barriers to accessing the Basic Package of Health Services (BPHS) in Afghanistan: Was the BPHS a success? Glob. Health 2016, 12, 71. [Google Scholar] [CrossRef] [PubMed]
- Musaiger, A.O. The food dome: Dietary guidelines for Arab countries. Nutr. Hosp. 2012, 27, 109–115. [Google Scholar] [PubMed]
- Musaiger, A.O.; Takruri, H.R. Food-based dietary guidelines for the Arab gulf countries. J. Nutr. Metab. 2012, 2012, 905303. [Google Scholar] [CrossRef] [PubMed]
- Promoting a Healthy Diet for the WHO Eastern Mediterranean Region: User-Friendly Guide. Available online: http://applications.emro.who.int/dsaf/emropub_2011_1274.pdf (accessed on 26 April 2019).
- Food and Agricultural Organization. Nutrition Country Profiles for Near East and Africa 2007. Available online: http://www.fao.org/ag/agn/nutrition/profiles_by_country_en. stm#neareast (accessed on 26 April 2019).
- Montagnese, C.; Santarpia, L. European food-based dietary guidelines: A comparison and update. Nutrition 2015, 31, 908–915. [Google Scholar] [CrossRef] [PubMed]
- Dietary Guidelines for Americans 2015–2020. Dietary Guidelines and MyPlate. Available online: http://www.choosemyplate.gov/dietary-guidelines (accessed on 26 April 2019).
- Joint Programme Initiative. A Healthy Diet for a Healthy Life, 2010–2030. Available online: https://era.gv.at/object/document/650/attach/Vision_paper.pdf (accessed on 26 April 2019).
- Galal, O. Nutrition-related health patterns in the Middle East. Asia Pac. J. Clin. Nutr. 2003, 12, 337–343. [Google Scholar] [PubMed]
- Obesity. Preventing and Managing the Global Epidemic. Report of a WHO Consultation (WHO Technical Report Series 894). Available online: https://www.who.int/nutrition/publications/obesity/WHO_TRS_894/en/ (accessed on 26 April 2019).
- International Conference on Nutrition. World Declaration on Nutrition and Plan of Action for Nutrition; FAO/WHO: Rome, Geneva, 1992; Available online: http://www.fao.org/3/u9260e/u9260e00.pdf (accessed on 26 April 2019).
- Swinburn, B.A.; Kraak, V.I. The global syndemic of obesity, undernutrition, and climate change: The lancet commission report. Lancet 2019, 393, 791–846. [Google Scholar] [CrossRef]
- Montagnese, C.; Santarpia, L. North and South American countries food-based dietary guidelines: A comparison. Nutrition 2017, 42, 51–63. [Google Scholar] [CrossRef] [PubMed]
- GCC. Total Population and Percentage of Nationals and Non-Nationals in GCC Countries (National Statistics, 2010–2017) (with Numbers). Available online: https://gulfmigration.org/gcc-total-population-percentage-nationals-foreign-nationals-gcc-countries-national-statistics-2010-2016-numbers/ (accessed on 26 April 2019).


{kind=link}
{kind=link}
{kind=link}
| North Africa (4) | Inhabitants (n) | Central East Africa (1) | Inhabitants (n) | Horn of Africa (2) | Inhabitants (n) | South Asia (3) | Inhabitants (n) | Western Middle East (5) | Inhabitants (n) | Arabian Peninsula (7) | Inhabitants (n) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Egypt 1 | 92,115,000 | Somalia 1 | 12,316,000 | Sudan 1 | 40,783,000 | Afghanistan | 29,200,000 | Syria 1 | 22,422,000 | Saudi Arabia | 32,552,000 | |
| Libya 1 | 6,545,000 | Djibouti 1 | 860,000 | Pakistan 1 | 213,707,000 | Lebanon | 4,421,000 | Yemen | 27,426,000 | |||
| Tunisia 1 | 11,446,000 | Iran | 79,926,000 | Jordan 1 | 10,053,000 | Oman | 4,560,000 | |||||
| Morocco 1 | 34,852,000 | Iraq 1 | 37,140,000 | Un. Arab Emirates | 9,121,000 | |||||||
| Palestine 1 | 4,706,000 | Qatar | 2,725,000 | |||||||||
| Bahrain | 1,501,000 | |||||||||||
| Kuwait | 4,184,000 | |||||||||||
| Total inhabitants per sub-region | 144,958,000 | 12,316,000 | 41,643,000 | 322,833,000 | 78,742,000 | 82,069,000 |
| Food Groups | WHO‒EMR: User Friendly Guide | Food Dome Dietary Guidelines for Arab Countries | Kingdom of Saudi Arabia | Lebanese Dietary Guidelines | Qatar Dietary Guidelines | Omani Guide to Healthy Eating | Afghanistan | Islamic Republic of Iran |
|---|---|---|---|---|---|---|---|---|
| Cereals/Grain Products and Tubers | 180 g/day: 90 g whole grain; 90 g “other” grains 30 g equivalent = 1 slice bread; ½ cup cooked pasta, rice, bulgar, or cereal; 1 cup dry cereal | 6–11 servings/day: ≥5.5 servings whole grain 1 serving = 1 slice bread; ¼ Arabic bread; ½ cup cooked cereals; 30 g dry cereal | 6–11 servings/day 1 serving = 1 slice bread (25 g), ½ cup of cereals, 1 slice of toast | 6 servings/day (with at least ½ being whole grain) based on 2000 kcal diet 1 serving = ¼ big loaf of Arabic whole-wheat pita bread; 1 slice bread; ½ cup rice, pasta, or noodles; 1 cup dry cereal (unsweetened) | ≥6 servings/day Substitute refined with whole and high-fibre grains. Choose grains prepared with little or no added fat, sugar or salt, read labels Avoid hydrogenated or trans-fat. | 6–11 servings/day 1 slice bread; ½ cup cooked rice, pasta, or cereal; prefer whole wheat, brown rice | 6 servings/day for a 2200 Kcal diet. 1 serving = ~140 kcal. ~ ¼ Naan (50 g piece); ~2/3 cup (125 g) cooked brown or white rice; 1 small potato boiled (160 g boiled weight), etc. | All types of bread (preferably whole), rice (brown, if available), macaroni, spaghetti, other pasta, barley |
| Fruits | 4 servings/day or 2 cups/day 1 serving = 1 medium fruit; ½ cup fresh fruit; 1 cup fruit juice | 3–5 servings/day 1 serving = 1 medium fruit; ¾ cup fruit juice | 2–4 servings/day 1 serving = 1medium fruit; ½ cup juice; ½ cup dried fruit | 2 servings/day 1 serving = 1 small fruit; 1 cup fruit juice; ½ cup dried fruit | 2–4 servings per day 1 serving = 1 medium fruit; ½ cup cut fruit; ½ fruit juice; ¼ cup dried fruit. Favour whole fruit over juices, choose often as snacks | 2–4 servings/day 1 serving = 1 cup raw or cooked; ½ cup fruit juice. Choose vitamin C-, vitamin A- and potassium-rich fruits. | 3 servings/day for a 2200 kcal diet. 1 serving = ~80 kcal | Apples, pears, citrus fruit, peaches, grapes; dried fruits; fruit juices |
| Vegetables | 5 servings/day or 2 ½ cups per day 1 serving = ½ cup raw or cooked; 1 cup leafy vegetable; ½ cup vegetable juice | 3–5 servings/day 1 serving = 1 cup raw; ¾ cup vegetable juice | 3–5 servings/day 1 serving = 1 cup raw or cooked; 1 cup juice | 2–3 servings/day 1 serving = 1 cup raw or cooked; 2 cup leafy vegetables; 1cup vegetable juice | 3–5 servings/day 1 serving = ½ cup cooked, fresh, raw, or canned; 1 cup green leafy vegetables | 3–5 servings/day Chose vegetables prepared with little or no added fat and salt. Choose vitamin C-, vitamin A- and iron/folic acid-rich vegetables. | 2.5 servings/day for a 2200 Kcal diet.1 serving = ~35 kcal | Green leafy and non-leafy vegetables |
| Milk & Dairy Products | 3 cup equivalent/ day 1 cup equivalent = 1 cup low-fat milk or yoghurt; 45 g low-fat natural cheese; 60 g processed cheese; 8 tbsp labneh | 2–3 servings/day 1 serving = 1 cup milk; 45 g cheese; 1 tbsp cream cheese | 2–4 servings/day 1 serving = 1 cup milk or labneh; 30 g cheese | 3 servings/day 1 serving = 1 cup low fat milk or dairy products to supply the daily recommended intake of calcium of 1000 mg/day based on 2000 kcal diet; 3 tbsp powdered milk; 45 g cheese; 8 tbsp labneh | 2 cup equivalents/day 1 cup eq. = 1 cup milk or yoghurt; 50 g cheese; 14 tbsp labneh Daily consumption of r low fat milk and dairy products. Choose vitamin D fortified milk | 1 serving/day 1 serving = 1 cup long-life, fresh, pasteurized, powdered milk or yoghurt; 45 g natural cheese; 60 g oz processed cheese, laban and kushk | 3.5 servings/day for a 2200 Kcal diet. 1 serving = ~70 kcal | Milk, cheese, yoghurt, yoghurt drink (doogh), kashk (a traditional dry milk product), ice cream |
| Meat & Vegetal Proteins | 160 g per day 1 serving = 30 g lean meat, poultry, or fish; 1 egg; ¼ cup cooked dry beans; 15 g nuts or seeds | 2–4 servings per day 1 serving = 50–80 g meat, chicken, or fish; 1 egg; ½ cup legumes and nuts | 2–3 servings per day 1 serving = 60–90 g red meat, chicken, or fish; ½ cup cooked legumes | 5–6.5 servings per day 1 serving = 30 g meat, poultry, or fish; 1 egg; 1 cup legumes; 15 g nuts or seeds | Eat a variety of fish at least 2 times a week. Chose skinless poultry and lean cuts of meat. Avoid processed meats. Chose legumes, nuts and seeds as alternative protein sources. Eat legumes daily. Choose legumes prepared with little or no added fat or salt | Meat: 1–2 servings/day 1 serving = 30 g red lean beef, lamb and camel, poultry, chicken. All fishes; 1 egg; 15 g oz nuts or seeds Legumes: 1 serving per day; ½ cup cooked lentils, beans or peas; ¼ cup cooked dry beans or tofu | Meat: 2 servings/day for a 2200 Kcal diet. 1 serving = ~70 kcal. Legumes: 1.5 servings/day for a 2200 Kcal diet. 1 serving = ~140 kcal. | Beef, veal, lamb, chicken, fish, canned tuna, shrimp, eggs Legumes, nuts including walnuts, almonds, pistachios, peanuts, hazelnuts |
| Oils | 6 tsp per day | None provided | “least amount per day” | Limited consumption | Limited Consumption | None provided | None provided | None provided |
| Salt, Fats & Sugars | Salt: no more 2,3 g/day. Use iodized salt for growth and brain development Fat: 18 g/day Sugar: 8 tsp/day | None provided | Use iodized salt, especially in cities that are not on the sea coast “Least amount per day” | Salt: no more 2.3 g/day for healthy people and to less than 1.5 g for people with hypertension, type 2 diabetes, chronic kidney disease, or over 50 years. Fat: 56–78 g per day Sugar: <10 tsp per day | Salt: <5 g/day Additional information on how to check food labels for the words salt or sodium. Distinguish “Foods high in salt” and “Foods low in salt” Fat: <3 g per 100 g Sugar: <5 g per 100 g | Salt: <5 g/day; Fat: 59 g per day Sugar: <10% total calories sugar | Salt: <5 g/day; Reduce simple sugars and substitute sweets with fruits. Remove visible fat from meat. Reduce processed meat consumption. | None provided |
| Water & Fluids | Men: 3.7 L/day Women: 2.7 L/day | “Sufficient quantity” | 1.5 L per day | 2–3 L per day | 2–3 L per day | Daily | Daily | Daily |
| Non Dietary Recommendations | WHO EMRO: User Friendly Guide | Food Dome Dietary Guidelines for Arab Countries | Kingdom of Saudi Arabia | Lebanese Dietary Guidelines | Qatar Dietary Guidelines | Omani Guide to Healthy Eating | Afghanistan | Islamic Republic of Iran |
|---|---|---|---|---|---|---|---|---|
| Physical Activity | 30 min/day of moderate PA | 30 min/day of moderate PA | 30–60 min/day | 30 min, 5 days a week | 30 min moderate PA, 5 days a week | Moderate PA: 30 min 5 days/week, Vigorous PA:20 min 3 days/week | 20–30 min PA/day | 30–40 min PA/day |
| Language | English | English, Arabic | English | English | English, Arabic | English | English | English |
| Food guide illustration shape | Plate (circle) | Food Dome | Healthy Food Palm | Lebanese Cedar (pyramid) | Tablecloth | Healthy Plate (circle) | Tablecloth | Pyramid |
| Food safety/Hygiene | Five keys for safer foods. Eat clean and safe food. | Ensure Safety of Food Eaten | Proper cleaning practices and food handling. Microbiological aspects of food safety, and practical matters related to safety precautions | Mothers and family members should practice hand washing-with soap and water at critical times | Wash your hands before handling food and often during food preparation, after going to the toilet. Wash and sanitize all surfaces and equipment used for food preparation. Protect kitchen areas and food from insects, pests and other animals | Mothers and family members should practice hand washing with soap and water at critical times | Washing hands and keeping chopping boards, plates, knives, etc. clean | |
| Safe water | Drink lots of clean water | Get your home tap water checked for microbial and mineral contamination. If it is not safe for drinking, drink safe bottled-water | Use clean and safe water for hand washing, drinking and food preparation | Untreated water from rivers and canals is not safe! Rainwater collected in clean tanks is safe as long as the tanks are protected from contamination from birds or other animals | Use clean and safe water for hand washing, drinking and food preparation | |||
| Healthy body weight | Maintain a healthy body weight | Maintain proper weight for height | Maintain an appropriate weight for your height | Enjoy and maintain a healthy body weight | Exercising regularly can help maintain a healthy body weight and high quality of life | Maintain a normal weight and stay healthy; you should eat adequately and have sufficient physical activity | ||
| Recommendations for specific population subgroups | Women of childbearing age, lactating women, strict vegetarians, lactose intolerance, elderly | Pregnant and lactating women, infants and preschool children, school children and adolescents, people aged 50 years | Pregnant, breastfeeding women, menopause, elderly, lactose intolerant, Vegetarians and strict vegans. Population groups most susceptible to food-borne illnesses (individuals with weakened immune systems, e.g., HIV-infected) | Pregnant, breastfeeding women, children, adolescents, vegetarians | Pregnant, breastfeeding women, children, adolescence, elderly | Pregnant, breastfeeding women, children, adolescence | ||
| Recommendations for specific diseases | Coronary heart disease, stroke, cancers, type 2 diabetes mellitus, cataract and macular degeneration, hypertension; dental caries | Diet-related diseases (heart disease, type 2 diabetes, hypertension, osteoporosis, obesity and cancer), undernutrition and micronutrient deficiencies | Obesity; CVD; hypertension, diabetes, dental caries, osteoporosis, rickets, micronutrient deficiencies | Obesity; CVD; diabetes, hypertension, obesity, cancer, dental caries, osteoporosis, nutrient deficiencies | Obesity; CVD; diabetes, hypertension, cancer, nutrient deficiencies, COPD | Obesity; CVD; hypertension, diabetes, obesity, cancer, dental caries, osteoporosis, nutrient deficiencies | Obesity; CVD; hypertension, BPCO, micronutrient deficiencies | Obesity; CVD; hypertension, diabetes, cancer, nutrient deficiencies |
| 1. | Maintain a healthy body weight |
| 2. | Be active |
| 3. | Limit intake of fats and oils |
| 4. | Limit intake of sugars, especially sweetened foods and beverages |
| 5. | Limit salt intake |
| 6. | Eat a variety of foods every day |
| 7. | Eat cereals, preferably whole grains, as the basis of most meals |
| 8. | Eat more vegetables and fruit every day |
| 9. | Eat legume-based dishes regularly and choose unsalted nuts and seeds |
| 10. | Eat fish at least twice a week |
| 11. | Consume milk/dairy products daily (preferably low-fat) |
| 12. | Choose poultry and lean meat |
| 13. | Drink lots of clean water |
| 14. | Eat clean and safe food |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montagnese, C.; Santarpia, L.; Iavarone, F.; Strangio, F.; Sangiovanni, B.; Buonifacio, M.; Caldara, A.R.; Silvestri, E.; Contaldo, F.; Pasanisi, F. Food-Based Dietary Guidelines around the World: Eastern Mediterranean and Middle Eastern Countries. Nutrients 2019, 11, 1325. https://doi.org/10.3390/nu11061325
Montagnese C, Santarpia L, Iavarone F, Strangio F, Sangiovanni B, Buonifacio M, Caldara AR, Silvestri E, Contaldo F, Pasanisi F. Food-Based Dietary Guidelines around the World: Eastern Mediterranean and Middle Eastern Countries. Nutrients. 2019; 11(6):1325. https://doi.org/10.3390/nu11061325
Chicago/Turabian StyleMontagnese, Concetta, Lidia Santarpia, Fabio Iavarone, Francesca Strangio, Brigida Sangiovanni, Margherita Buonifacio, Anna Rita Caldara, Eufemia Silvestri, Franco Contaldo, and Fabrizio Pasanisi. 2019. "Food-Based Dietary Guidelines around the World: Eastern Mediterranean and Middle Eastern Countries" Nutrients 11, no. 6: 1325. https://doi.org/10.3390/nu11061325
APA StyleMontagnese, C., Santarpia, L., Iavarone, F., Strangio, F., Sangiovanni, B., Buonifacio, M., Caldara, A. R., Silvestri, E., Contaldo, F., & Pasanisi, F. (2019). Food-Based Dietary Guidelines around the World: Eastern Mediterranean and Middle Eastern Countries. Nutrients, 11(6), 1325. https://doi.org/10.3390/nu11061325